The Architectural Failure Underneath Modern Medicine
What gets missed when we read biology as a parts list, and what becomes possible when we read it as architecture
For four years I have been working on a problem that almost no one has named clearly.
Modern clinical genetics has been failing patients for decades, and the reason is structural. Standard genetic interpretation reads variants in isolation, scored against population averages derived from cohorts that may not represent the individual patient sitting in front of the doctor. That framework cannot distinguish a variant that drives disease from a variant that is an evolutionary adaptation to a specific environmental pressure. It cannot account for the architectural interactions between variants that determine how biology actually behaves in real molecular systems.
The result is population-averaged guidance for individuals who are not the population average, delivered at clinical scale for thirty years.
Adverse drug reactions cost the United States around 30 billion dollars a year. Roughly one in ten hospitalizations for older adults comes from a medication problem. Two patients with similar genetics routinely have opposite reactions to the same drug. The field has been treating that variability as random noise when it is actually the signal of a deeper interpretive failure.
The deeper failure is the framework itself. Reading biology as a parts list rather than as an architecture.
The Architectural Reframe
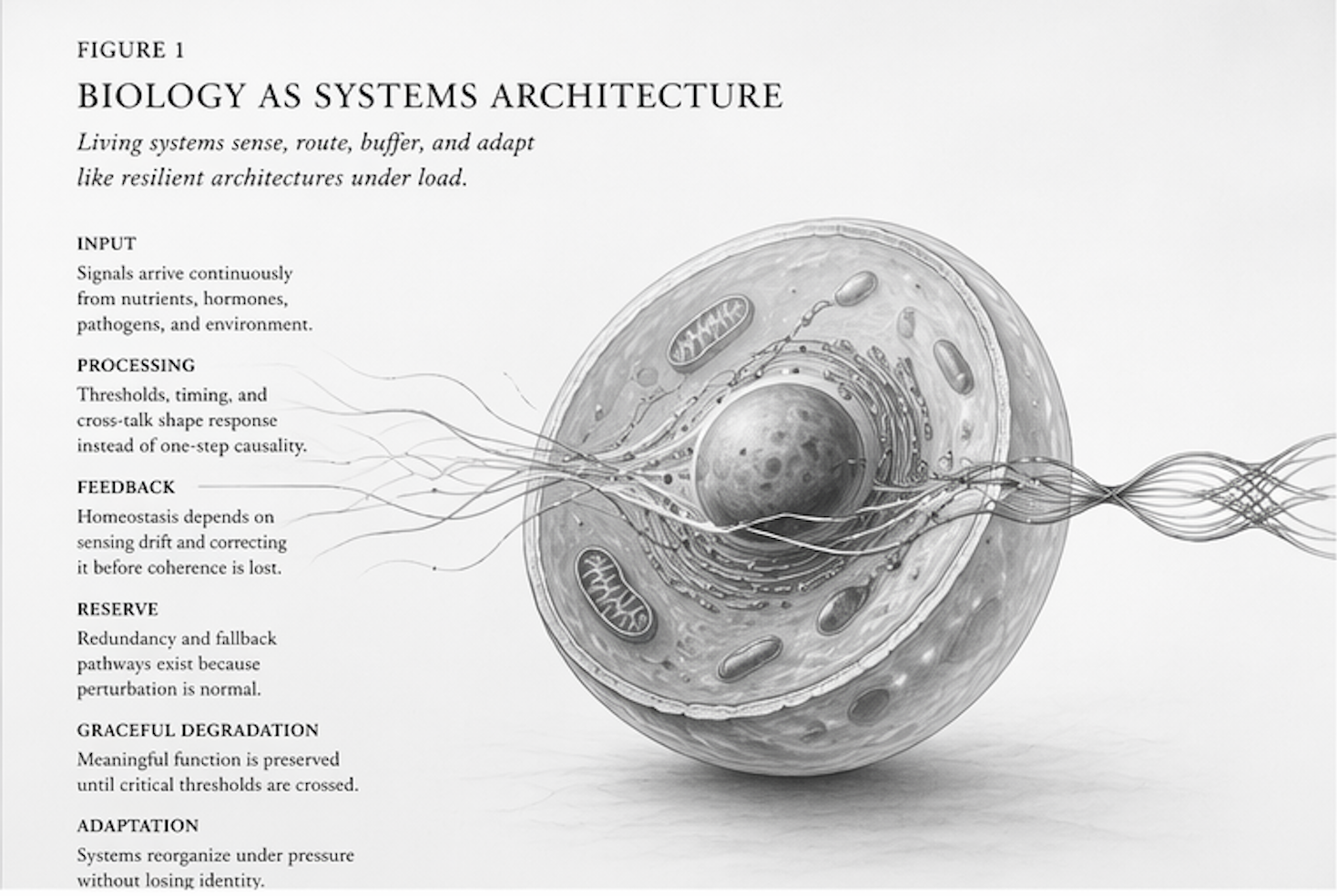
Biology is not a collection of independent genetic parts. It is a constraint network where variants interact with each other, with ancestry, with environmental context, and with the larger system that holds all of it together.
The textbook case is sickle cell. For decades, modern medicine has treated the sickle cell variant as straightforwardly pathogenic. But the variant is in the human genome at the frequencies it sits at for a specific reason. People who carry one copy of the variant get around 80 percent protection from severe malaria. That is one of the strongest evolutionary pressures in the recent history of the human species. The same variant produces disease in one configuration and produces survival advantage in another. Whether it shows up as illness or as protection depends on the evolutionary architecture around it, the environment the patient lives in, and the molecular interactions that determine how the variant actually behaves.
Standard genetic interpretation cannot read any of that. It scores the variant in isolation, against a population average, and produces a binary clinical label.
The reframe is that biology has been telling us all along that variants live inside an evolutionary architecture, and reading them without that architecture is the source of a great deal of misclassification.
I wrote about this in The Adaptation Paradox: How Evolution's Gifts Became Medicine's Problems. The book makes the case that many of the variants currently labeled pathogenic by standard testing are actually evolutionary adaptations to specific environmental pressures, miscategorized because the interpretive framework cannot read evolutionary context.
The framework has been failing because the framework has been reading biology wrong.
What Becomes Possible
When you read biology as architecture, the questions change.
Variant interpretation becomes context-aware rather than population-averaged. Drug response prediction becomes individual-specific rather than cohort-averaged. Trial enrollment becomes stratified by metabolic and genetic architecture rather than treating heterogeneous populations as homogeneous. Adverse drug reactions become predictable from the architecture rather than treated as random variability.
The infrastructure to read biological architecture at clinical scale is what NomosLogic operates. Whole-genome resolution in production. Multi-omic clinical data integration. Evolutionary medicine integrated into clinical decision support. Every clinical assertion the platform produces is rule-based, reproducible, and cryptographically anchored. The decision layer is deterministic. The translation layer is constrained by the substrate.
That distinction matters. AI in clinical genomics has produced impressive demonstrations and a lot of unreliable output. The reason is that probabilistic AI systems applied to interpretive frameworks that are themselves wrong produce sophisticated-looking outputs that inherit the underlying interpretive failures. Building deterministic infrastructure underneath the AI surface is what makes the output auditable. The AI helps render the deterministic findings into language that humans can engage with. The AI does not author the findings.
This is the architectural commitment that distinguishes infrastructure from interface.
The Work Ahead
The architectural reframe opens a lot of questions that the field needs to work through together. How do we integrate evolutionary context into clinical decision support without producing complexity that overwhelms the clinical workflow? How do we run clinical trials that account for individual genetic architecture rather than averaging across heterogeneous populations? How do payer systems adapt to prescribing guidance that is patient-specific rather than population-averaged? How do regulatory frameworks evaluate deterministic infrastructure differently from probabilistic AI tools? How do partnerships across pharma, payer, provider, and research surfaces compound the value of architecture-aware interpretation?
I have spent four years building infrastructure to answer the first version of these questions at clinical scale. The infrastructure is in production. The science is published. The architectural argument is increasingly being recognized.
The work ahead is collaboration.
I am looking to work with operators who recognize that the interpretive framework underneath clinical genomics is the constraint, not the data layer above it. Pharma research teams running into the limits of population-averaged response prediction. Payer organizations trying to design coverage around architecture-aware prescribing. Health systems building clinical decision support that needs to account for individual genetic architecture. Academic collaborators working on evolutionary medicine, distributed constraint biology, and the foundations of deterministic clinical interpretation. Investors who understand that infrastructure with this level of architectural commitment compounds across multiple application surfaces.
The mission is the structural rebuild of how medicine reads biology. Personalized care should not be a luxury for the wealthy. It should be the standard of care for every patient. Cures for the incurable. Accurate prescribing for populations that have been failing standard care for decades. Drug pricing that reflects what actually works in actual people.
Building infrastructure at this altitude is not a one-operator problem. The architecture exists. The platform is in production. The science is being validated. What scales the impact is the operators who recognize the architectural reframe and want to build alongside it.
If that is you, I want to talk.
You can find me at https://x.com/NomosLogic.The platform is at nomoslogic.com. Both books are available on Amazon. The Adaptation Paradox: How Evolution's Gifts Became Medicine's Problems documents the misclassification problem in standard clinical genetics. Deterministic Convergence: Biological Systems, Architecture, and the Search for Hidden Order documents the architectural reframe and its empirical foundation.
Matt Hardy
Founder and CEO, NomosLogic