The case for deterministic infrastructure as the foundation of clinical AI
Modern medicine has not been failing because the science is missing. It has been failing because the framework underneath clinical decision-making has been reading biology incorrectly.
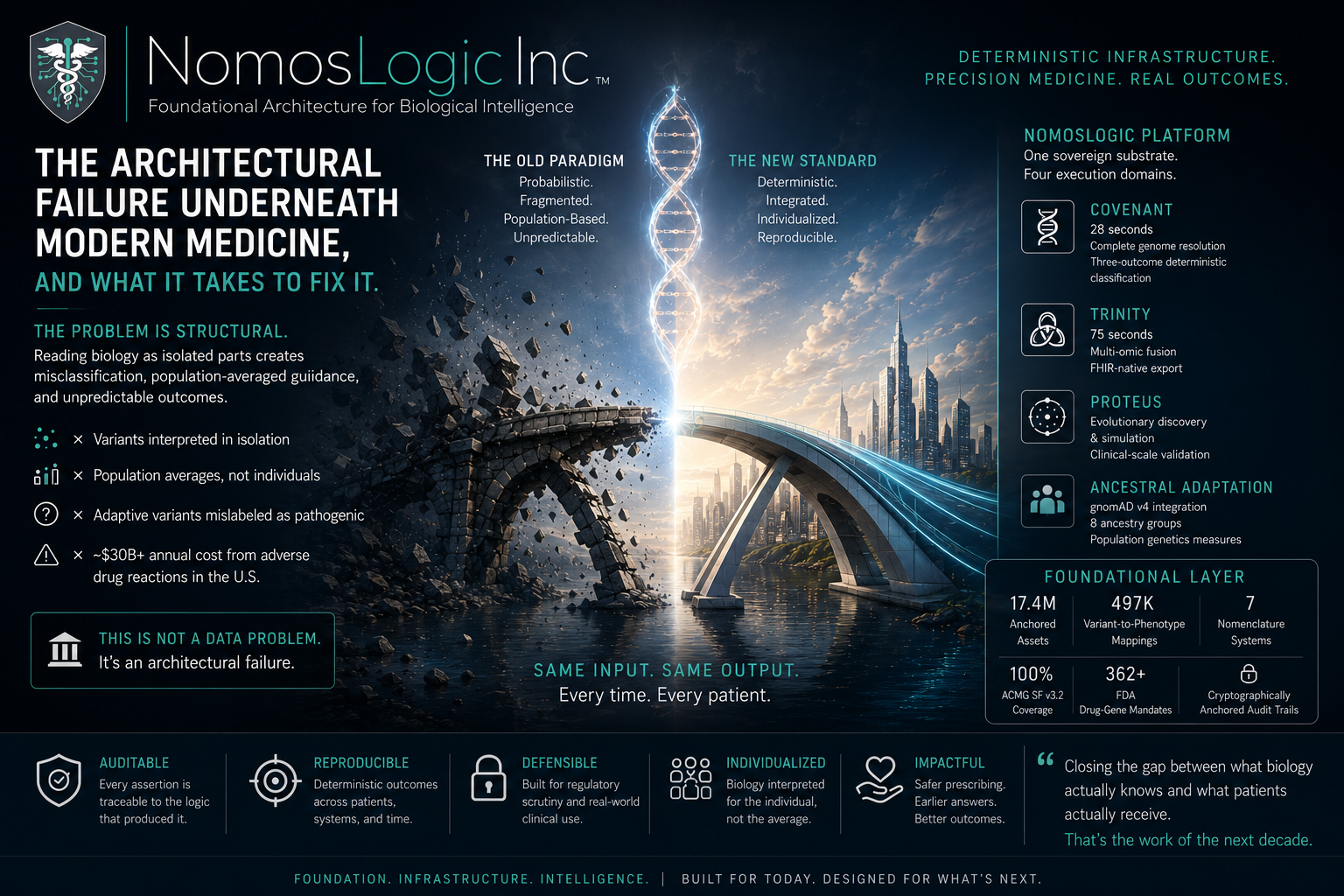
The cost is measurable.
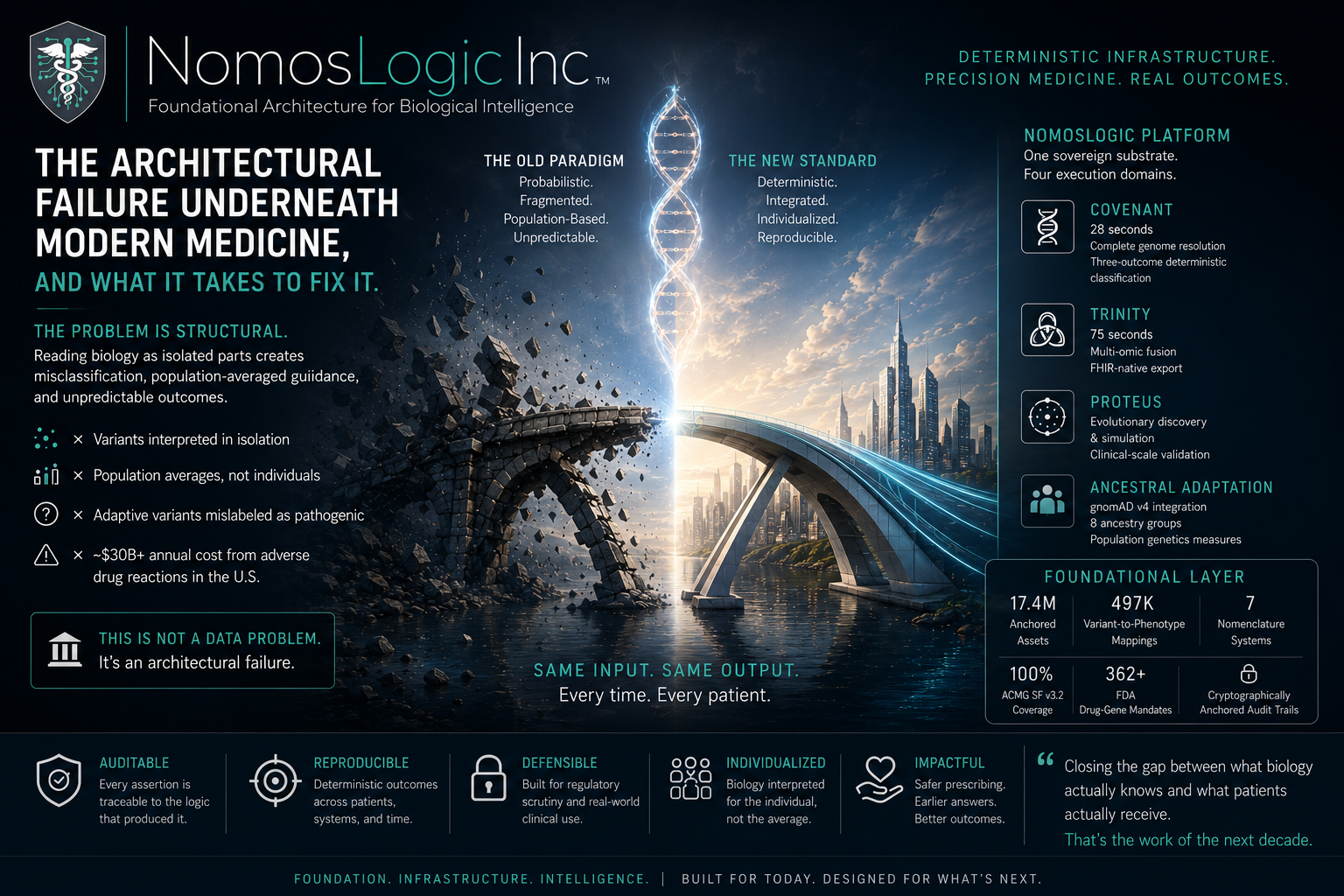
Adverse drug reactions cost the United States roughly $30 billion annually. Medication-related complications account for a significant percentage of hospitalizations among seniors. Two patients with highly similar genetic profiles routinely produce opposite responses to the same therapy, yet modern clinical genetics still treats much of that variability as noise rather than as evidence of a deeper architectural failure.
The problem is structural.
Clinical genetics has largely interpreted biology as a parts list. Variants are scored in isolation against population-derived averages that often fail to represent the individual patient sitting in front of the clinician. The framework struggles to distinguish pathogenic variation from evolutionary adaptation, and it cannot adequately model the distributed interactions between variants that determine how biological systems actually behave.
The result is a system that produces population-averaged guidance for individuals who are not the population average.
This is not a data problem.
Whole genome sequencing is increasingly affordable. Pharmacogenomic testing continues to expand. Multi-omic data is becoming more accessible every year. The limitation is not the absence of data, but the interpretive framework used to convert that data into clinical decisions.
The Principle of Deterministic Convergence
Biology is not a collection of isolated parts. It is a distributed constraint network where variants interact with one another, with ancestry, with environment, and with the larger molecular systems surrounding them.
When biology is interpreted as disconnected components, critical system-level behavior disappears into statistical noise. When biology is interpreted architecturally, those same patterns become legible.
The principle of deterministic convergence formalizes this idea.
Biological systems converge toward stable architectural states determined by distributed molecular constraints. Those convergence properties are reproducible across unrelated clinical domains when the same analytic framework is applied consistently.
The framework has now been validated across six unrelated clinical systems:
cardiovascular
neurological
oncological
renal
metabolic
hematological
The same analytic operation produced consistent convergence behavior across all six domains. That level of universality suggests the presence of a foundational architectural principle rather than a domain-specific statistical artifact.
The framework is detailed in the reference work Deterministic Convergence: Biological Systems, Architecture, and the Search for Hidden Order. Its clinical and evolutionary implications are expanded further in The Adaptation Paradox: How Evolution’s Gifts Became Medicine’s Problems, which explores how many variants currently labeled pathogenic may instead represent evolutionary adaptations to historical environmental pressures.
Both works are public and open to testing, extension, criticism, and refutation by the broader scientific community.
Why Probabilistic Clinical AI Cannot Reach the Floor
Most clinical AI systems operating today remain probabilistic at their core.
A probabilistic model trained on a structurally flawed interpretive framework will inherit those same structural errors. If adaptive variants are systematically misclassified as pathogenic at the data interpretation layer, larger models and additional compute simply reproduce those errors at scale.
More data does not resolve an architectural flaw. More compute does not resolve an architectural flaw.
The interpretive substrate itself must change.
Equally important, probabilistic infrastructure faces growing regulatory and auditability constraints that the industry has not fully reckoned with yet.
When regulators, payers, or clinicians ask:
“Show me the exact logic that produced this recommendation for this patient.”
systems built on deterministic, traceable infrastructure will be able to answer directly.
Systems that cannot produce reproducible and auditable decision pathways will face increasing scrutiny as genomic medicine moves deeper into regulated clinical workflows.
Deterministic infrastructure is the architectural commitment that survives that transition.
Same input. Same output. Every time.
Every clinical assertion is:
rule-based
reproducible
traceable
cryptographically anchored to the logic that produced it
AI still plays a critical role, but at the interpretation and communication surface where it belongs, not at the call itself.
That distinction is not cosmetic. It is the structural property that makes clinical infrastructure auditable, defensible, and durable under the regulatory conditions medicine is moving toward.
What Is Operating Today
NomosLogic operates a deterministic molecular medicine infrastructure layer designed to bridge clinical genomics, consumer genomics, payer systems, and pharmaceutical research from a unified substrate.
Four engines currently operate on the platform through the Hardy Bridge nomenclature translation layer:
COVENANT resolves complete human genomes in approximately 28 seconds using deterministic three-outcome classification.
TRINITY fuses multi-omic clinical data with FHIR-native export in approximately 75 seconds.
PROTEUS performs evolutionary simulation and systems-level discovery across large-scale molecular datasets.
Ancestral Adaptation integrates gnomAD v4 population data across eight ancestry groups to distinguish adaptive variation from pathogenic variation using population genetics measures.
The underlying molecular reference layer currently contains:
17.4 million anchored assets
497,000 variant-to-phenotype mappings
seven harmonized nomenclature systems
full ACMG SF v3.2 secondary findings coverage
and more than 362 FDA drug-gene mandates
Every clinical assertion generated by the platform remains deterministic, reproducible, and cryptographically auditable.
The deterministic standard for clinical infrastructure did not meaningfully exist at scale inside modern genomics. NomosLogic was built specifically to address that gap.
The Horizon
The next decade of clinical infrastructure will be defined by which systems can satisfy the coming demands for:
interpretability
auditability
reproducibility
and individualized biological precision
Deterministic convergence provides the framework. Deterministic infrastructure provides the foundation. The platform is the implementation.
The real challenge in modern medicine is no longer generating biological data. It is closing the gap between what biology already knows and what the patient sitting in front of a clinician actually receives.
That requires infrastructure capable of translating molecular complexity into reproducible clinical action at scale.
The mission is larger than software.
It is the structural rebuilding of how clinical decisions are made:
personalized care beyond population averages
safer prescribing across diverse populations
earlier identification of biological risk
and precision medicine accessible beyond boutique healthcare systems
The systems that recognize the architectural argument as the argument are the systems that will define what comes next.