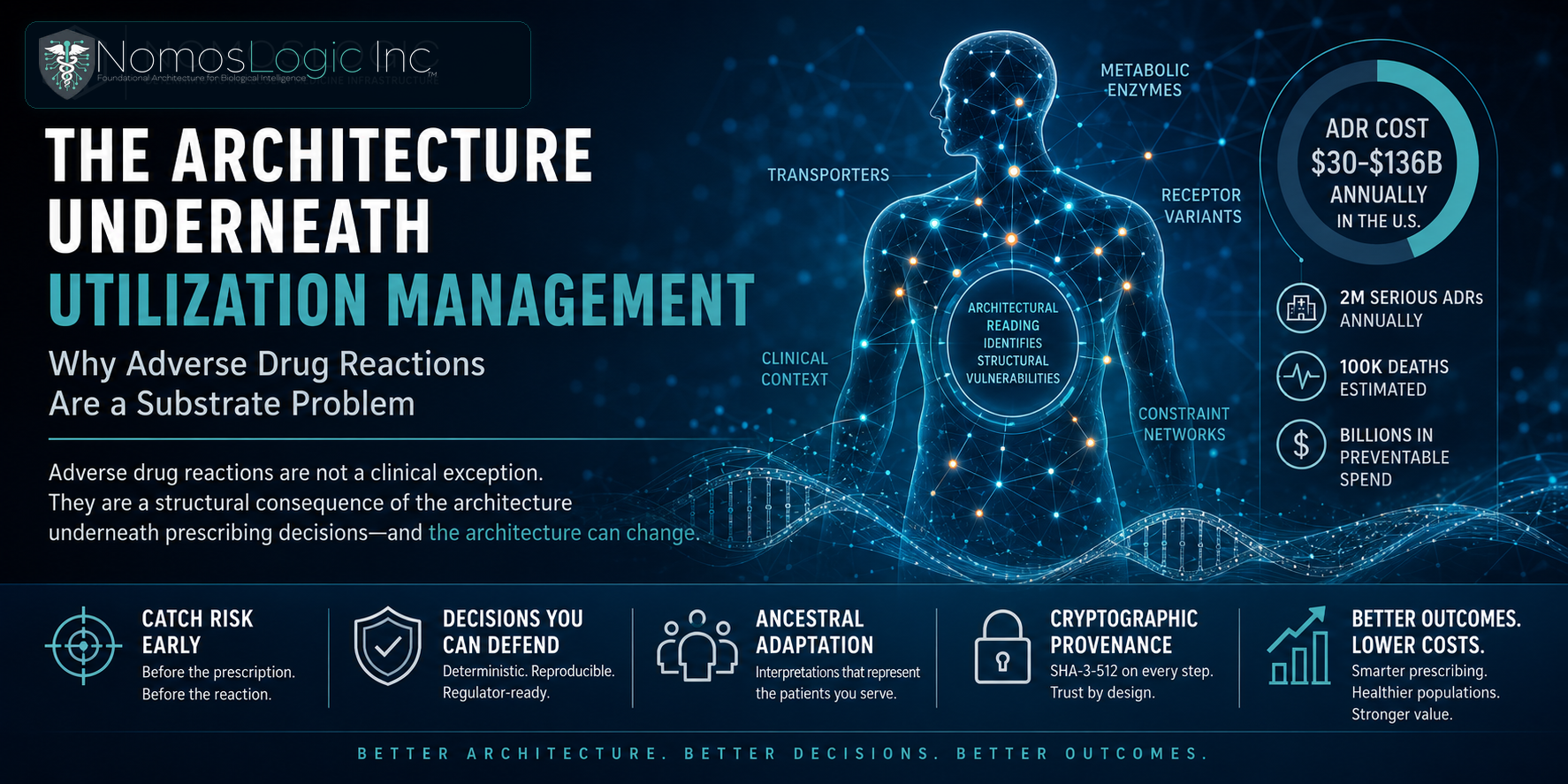
Adverse drug reactions are caught most cost-effectively at the prescribing decision point, before the prescription is filled and before the reaction occurs. Catching them at the claims-after-adverse-event step is operationally where current infrastructure operates, and the cost surface compounds because the architecture upstream cannot read what it needs to read.
For payer medical directors thinking about where infrastructure investment compounds, the prescribing decision point is the surface where architectural reading conditioned on ancestry produces measurable changes in utilization, member outcomes, and the clinical defensibility of utilization management decisions that the regulatory and value-based contract environment is increasingly going to require.
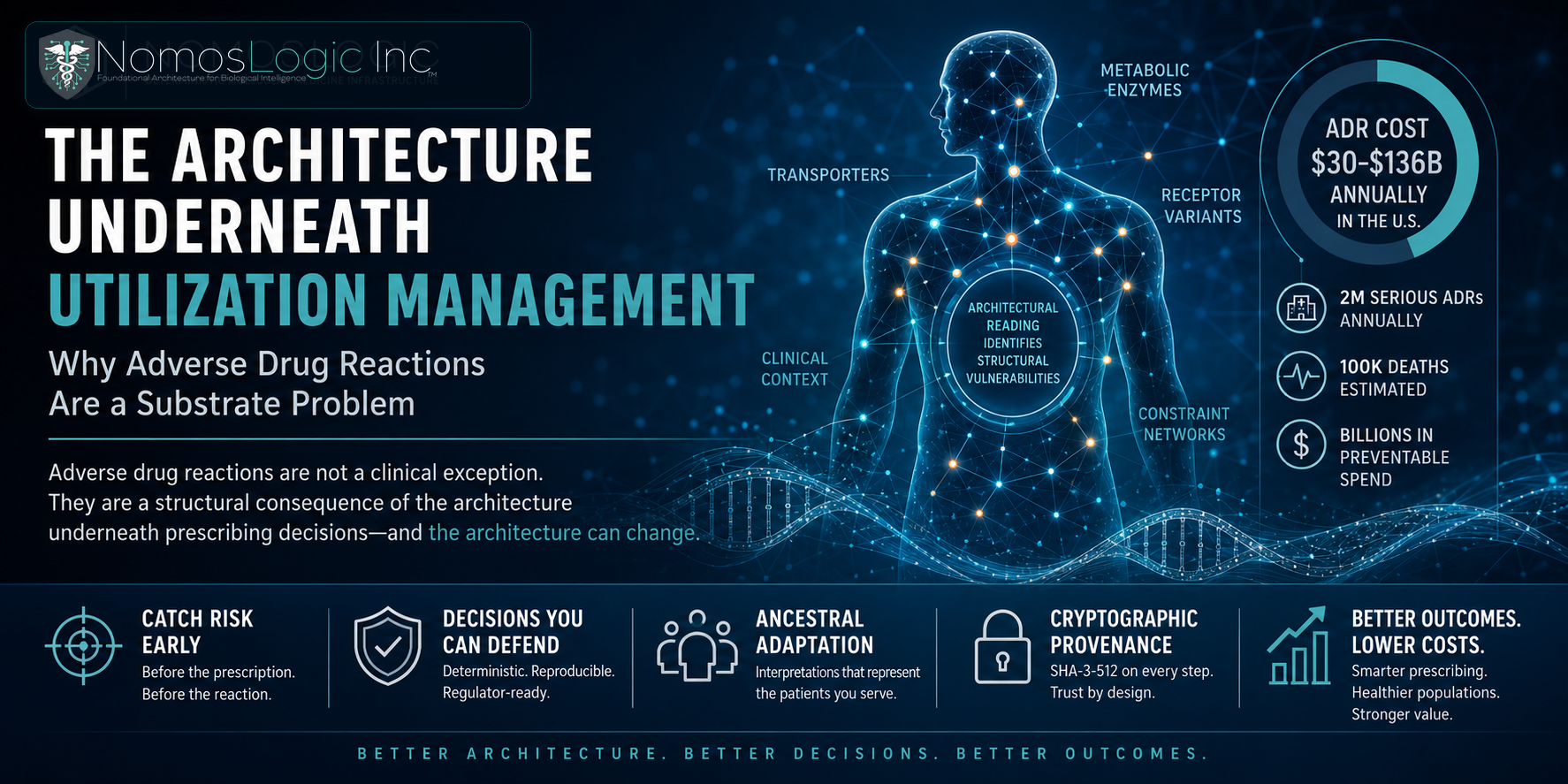
The substrate underneath the decisions is what determines whether the decisions can be defended. NomosLogic is the substrate. The architecture is the decision layer the field has been waiting for.