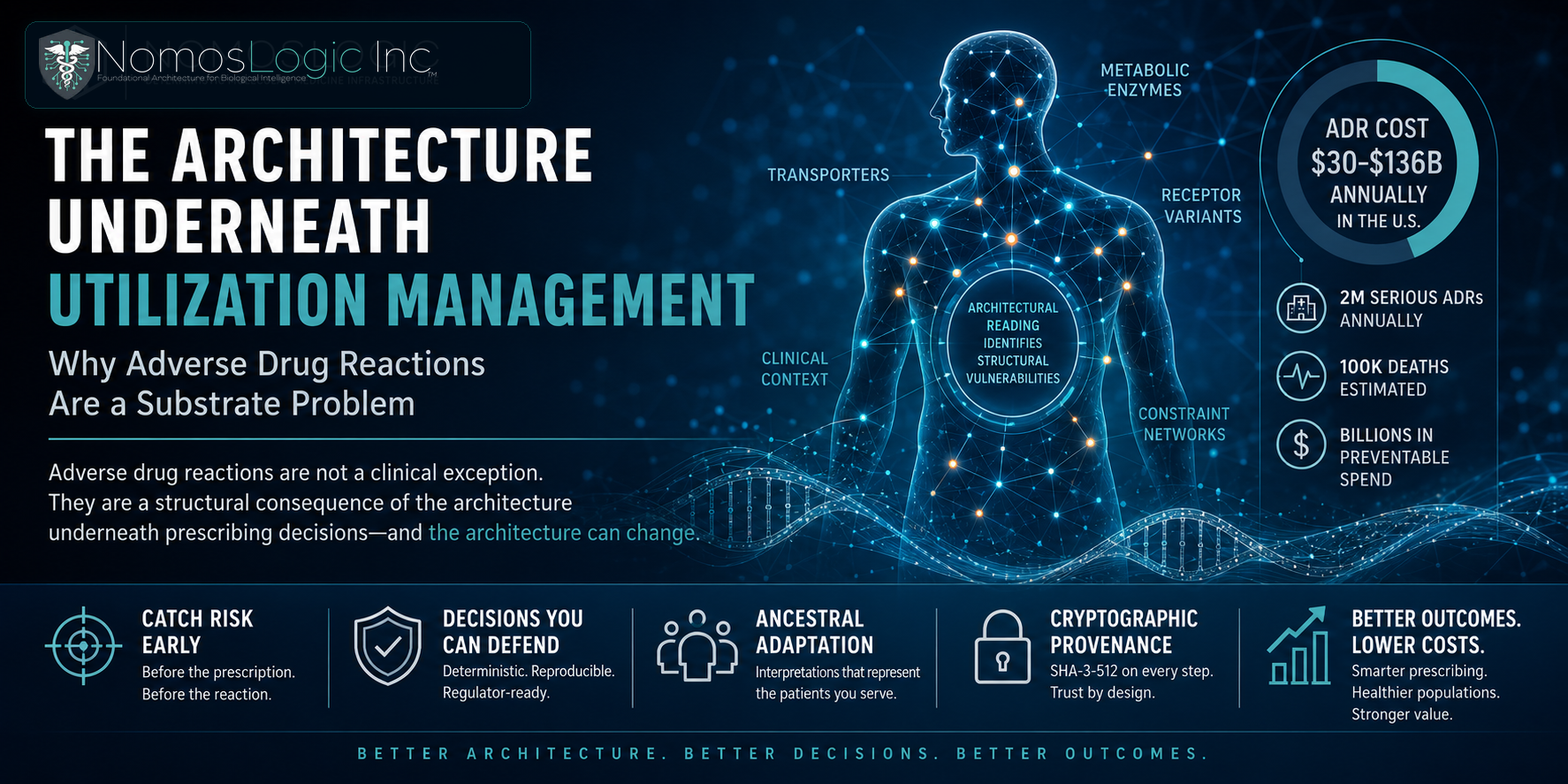
The Architecture Underneath Utilization Management
Why Adverse Drug Reactions Are a Substrate Problem
NomosLogic is deterministic molecular medicine infrastructure. This article is for the payer medical directors and chief medical officers who make the utilization management decisions that current pharmacogenomic infrastructure cannot support defensibly. It argues that adverse drug reactions are not a clinical exception to manage downstream. They are a structural consequence of the architecture underneath prescribing decisions, and the architecture can change.
The clinical defensibility problem
Every utilization management decision a payer organization makes carries a defensibility surface. Prior authorization denials, medical necessity determinations, formulary tier assignments, step therapy protocols. Each one has to hold up under three forms of scrutiny: the patient who experiences the outcome, the regulator who reviews the decision pattern, and the value-based contract counterparty who measures the population-level result.
The current pharmacogenomic decision support infrastructure deployed across most payer organizations cannot produce decisions that hold up cleanly under all three. The reason is architectural.
Most variant interpretation systems in production today operate on population-averaged scoring against reference cohorts that were built when the available samples were European-ancestry-dominant. The same patient genomic profile produces different recommendations depending on which reference database the scoring runs against, which version of the database is current, and whether the system has recent labeling for the drug-gene combination in question. Different systems produce different outputs for the same patient. Different runs of the same system produce different outputs when model state has shifted between runs.
For a payer medical director, that property means the clinical recommendation the system produces cannot be cleanly replayed when the decision is questioned six months later. The output that justified the prior authorization approval at the time of decision may not be reproducible from the same inputs at the time of review. That is not a documentation problem. It is an architectural property of probabilistic systems, and it breaks the chain of clinical defensibility that utilization management requires.
The cost surface that compounds underneath
Adverse drug reactions cost the US healthcare system at least $30 billion per year in direct medical spending, and the upper-bound estimates in the systematic review literature extend to $136 billion per year when indirect costs, productivity loss, and outpatient settings are included. The FDA's Center for Drug Evaluation and Research estimates approximately 2 million serious ADRs annually in the United States, contributing to roughly 100,000 deaths.
Those numbers are not background context. They are the cost surface that payer organizations absorb when prescribing decisions produce reactions that the system could have surfaced before the prescription was filled. Failed therapy cycles. Emergency department utilization. Hospital admissions. Behavioral health utilization downstream of psychiatric medication mismatches. Chronic care complications from cardiovascular and metabolic drug interactions that pharmacogenomic decision support would have caught if the architecture underneath it had been adequate.
For a plan covering 10 million members, the proportional share of the national ADR cost surface is large enough that even small improvements in prescribing accuracy produce material reductions in utilization. For larger plans, the surface is correspondingly larger. The question is not whether the cost is real. The question is whether the infrastructure deployed at the prescribing decision point is capable of catching the mismatches that produce the cost.
What architectural reading produces that population averaging cannot
The constraint relationships that determine whether a medication will succeed or fail in a specific patient are not properties of individual variants. They are properties of the architecture those variants participate in. CYP metabolism does not happen in isolation. Drug response depends on the interaction of metabolic enzymes, transporter proteins, receptor variants, and clinical context. The architecture is what determines the outcome.
Population-averaged scoring collapses that architecture into per-variant probability distributions. Architectural reading represents the constraint relationships explicitly. The two approaches produce different categories of output. Probability distributions are statistical predictions over individual variants. Architectural readings are structural descriptions of how the patient's constraint network will respond to the medication.
For payer medical directors, the operational difference is in what each output enables. Statistical predictions support recommendations with confidence intervals. Architectural readings support recommendations with auditable reasoning that traces from the patient's genomic profile through the constraint relationships to the predicted outcome. The first produces a number. The second produces a decision pattern that can be examined, replayed, and defended at the per-patient level.
That distinction matters because utilization management decisions are not made in the abstract. They are made about specific patients, and they are reviewed when specific outcomes deviate from what was expected. The system that supports the decision has to support the review.
Ancestral adaptation as a clinical defensibility property
The reference cohorts underneath most variant interpretation infrastructure remain European-ancestry-dominant in 2026. Plan populations are not. The gap between the reference data the scoring was built against and the actual ancestry composition of the membership is where clinical defensibility breaks for diverse populations specifically.
A medical director approving prior authorization for a pharmacogenomic-guided psychiatric medication regimen in a member whose ancestry is Han Chinese, or Yoruba, or admixed American with significant Indigenous heritage, is making a decision supported by reference data that does not represent the member's actual genomic context. The recommendation may be statistically reasonable for the population the system was trained on. It may also be structurally degraded for the actual patient.
That gap has clinical consequences that show up in the outcome data. Plan populations diverging from European-ancestry reference cohorts experience pharmacogenomic mismatches at higher rates than the system predicts. The cost surface for those populations compounds disproportionately, and the regulatory exposure compounds with it as health equity becomes a measured property of plan performance.
Architectural reading conditioned on ancestry is the property that closes the gap. The constraint relationships are read against the population the patient actually belongs to rather than against the reference cohort the scoring infrastructure inherited. The interpretation is recovered for the patients whose interpretation current infrastructure systematically degrades.
What deterministic infrastructure enables that current systems cannot
NomosLogic operates molecular medicine infrastructure that runs on three engines. COVENANT is the deterministic variant resolution engine that anchors every finding with cryptographic provenance. TRINITY is the multi-omic fusion engine. PROTEUS reads architectural structure in constraint networks through deterministic evolutionary simulation. Underneath every engine, Hardy Bridge translates across the 40-plus nomenclature systems that fragment current variant interpretation, and ancestral adaptations contextualize the architectural reading for the populations the patient actually belongs to.
The relevant property for payer utilization management is that the output is deterministic by construction. Identical inputs produce identical outputs across independent runs. Every finding carries SHA-3-512 cryptographic provenance on every analytical step. Encryption at rest is HMAC-SHA256. Exports carry a hashed manifest that traces every result back to the analytical step that produced it.
For a medical director, that property means the recommendation that justified a utilization management decision at the time of decision can be replayed exactly at the time of review, six months or six years later. The clinical defensibility surface is structural rather than procedural. The decision pattern can be examined under regulatory review, value-based contract performance review, and member appeal review without requiring reconstruction of model state that no longer exists.
That structural defensibility is what current probabilistic infrastructure cannot produce, and it is the property that makes architectural reading deployable at the prescribing decision point inside payer workflow.
The decision point that matters
Adverse drug reactions are caught most cost-effectively at the prescribing decision point, before the prescription is filled and before the reaction occurs. Catching them at the claims-after-adverse-event step is operationally where current infrastructure operates, and the cost surface compounds because the architecture upstream cannot read what it needs to read.
For payer medical directors thinking about where infrastructure investment compounds, the prescribing decision point is the surface where architectural reading conditioned on ancestry produces measurable changes in utilization, member outcomes, and the clinical defensibility of utilization management decisions that the regulatory and value-based contract environment is increasingly going to require.
The substrate underneath the decisions is what determines whether the decisions can be defended. NomosLogic is the substrate. The architecture is the decision layer the field has been waiting for.